Redefining COVID-19 disease

Preface: I‘m not a doctor or microbiologist nor a professional researcher. I’m just a fairly smart ‘layman’ with a passion for medicine and a desire to stop this disease or find a treatment. I’m probably using imperfect terminology, but what follows is my attempt to make sense of some new data and evidence that this disease may not be what assumed.
Over the last few days there’s been a bit of an undercurrent of chatter about the need to look at this disease from a different angle. Much of what follows is a combination of listening carefully to that undercurrent, filtering the noise, and then connecting some dots.
On Saturday April 4, 2020, I wrote a Facebook post with the beginning of an understanding of what I believe is going on with COVID-19 and how it’s attacking the body. In that post I was hypothesizing that this disease is in fact a blood disease not a respiratory one. I was starting to think that there is no pneumonia or ARDS in most cases. I was starting to understand that iron was somehow involved in this. And critically to this moment, that positive pressure ventilation was possibly doing more damage than good.
In the days since I wrote that post it’s become increasingly clear I was on the right track and that we may be on the cusp of a bigger understanding of this disease and perhaps, dare I say, even cracking the nut that is COVID-19.
High-Level Hypothesis
This article is a layman’s attempt at finding a common thread that explains much of what is being observed in terms of the symptoms, risk factors and treatments of this disease.
Up front, the hypothesis is that COVID-19 is actually a blood disease that attacks red blood cells and releases iron — killing through a combination iron poisoning and oxygen deprivation.
My goal is to get this hypothesis into the right hands that so that it can be picked apart at a more scientific level, or even better, be confirmed so that treatments can be developed as quickly as possible.
But let’s backtrack. What do we currently know about COVID-19 and the disease progression:
Common Symptoms:
Dry Cough, Fever, Headaches, Shortness of Breath (but notably — not generally an inability to draw breath), Sore “bones”, extreme fatigue, loss of smell and taste.
And non-localized ground-glass-opacity visible throughout lungs visible in CT scans.
Lethal Symptoms:
Multiple organ failure leading to death.
Multiple organ failure leading to death.
Risk factors leading to higher liklihood of serious / lethal outcomes:
Blood Type
Age
Gender
Hypertension
Diabetes
Obesity
Blood Type
Age
Gender
Hypertension
Diabetes
Obesity
Treatments of promise:
Hydroxychloroquine / Chloroquine / Quinine (also SARS-COV1 2004, 2005, 2008, 2009)
+ Zinc
+ Azithromycin
Intravenous Vitamin C
Blood Transfusions
Remdesivir / Favipiravir / Antivirals
BCG Vaccination
Hydroxychloroquine / Chloroquine / Quinine (also SARS-COV1 2004, 2005, 2008, 2009)
+ Zinc
+ Azithromycin
Intravenous Vitamin C
Blood Transfusions
Remdesivir / Favipiravir / Antivirals
BCG Vaccination
A Unifying Theory
Let’s begin connecting everything above into a unified theory.
Up until recently it’s been widely assumed that the coronavirus COVID-19 is a respiratory disease, i.e. a disease of the lungs. I would like to argue that, while the lungs do in fact play a crucial role in the disease and are very likely the place where the virus starts its attack and replicates itself. It’s not in fact the lung damage that kills, or at least not alone.
In layman’s terms, you get infected with with SARS-COV-2 (the “coronavirus”) when you breathe it into your lungs. From there it uses its spike protein to attach to the ACE2 receptors on your lung cells, the virus then injects its RNA proteins into the cell, at which point the cell’s replication machinery uses the virus RNA to create new copies of the virus. This is well-understood and I have no reason to believe this isn’t the case.
This obviously damages the lungs, but I don’t think that’s what’s causing the “ground glass opacities” we see in CT scans. More on this later. I actually believe it’s a fairly run-of-the-mill viral lung infection at this point. Doing some damage, but not deadly amounts in most cases.
Here is where this new theory starts to diverge from the mainstream understanding of this disease. At this point I believe the rapidly replicating virus, through some not fully understood method, starts to attack the red blood cells of our body. Specifically, it binds to the hemoglobin of our red blood cells.
The results showed the ORF8 and surface glycoprotien could bind to the porphyrin, respectively. At the same time orf1ab, ORF10, and ORF3a protiens could coordinate an attack of the heme on the 1-beta chain of heboglobin to dissociate the iron from the porphyrin. This attack will cause less and less hemoglobin that can carry oxygen and carbon dioxide. — from ChemRxiv study
I believe this is where most of the damage to our organs occurs. Because, in doing so, it basically knocks the highly toxic forms of iron (fe2+, fe3+) inside the red blood cell out. This free-floating, highly-reactive, positively-charged element then binds nearly immediately to the nearest positively charged molecules/elements it bumps into. Those molecules could very well be part of a heart muscle, or liver, lung, olfactory, or even brain.


I also hypothesize that since it’s the iron that the oxygen binds to when we breathe, the oxygen is also being released into our bloodstream, no longer bound inside our red blood cells. What does that do to our body?
Basically, this virus is triggering the release of huge amounts of dangerous, even deadly, free floating iron in our blood serum, (and also oxygen?).
Now again, I’m just a layman, and I’m sure the above and below are massive simplifications. But let’s continue and connect some dots.
How does this blood infection theory help explain symptoms?
Let’s start at the top.
Common symptoms:
Obviously the virus is initially attacking the lungs, so of course we cough. But in addition to the initial infection site, it appears that with the virus attacking the blood hemoglobin and blocking the lung’s ability to exchange oxygen and carbon dioxide, the lungs take further damage causing shortness of breath.
Common symptoms:
Obviously the virus is initially attacking the lungs, so of course we cough. But in addition to the initial infection site, it appears that with the virus attacking the blood hemoglobin and blocking the lung’s ability to exchange oxygen and carbon dioxide, the lungs take further damage causing shortness of breath.
In my hypothesis this excess iron is also spreading throughout the body and causing damage everywhere, and so we lose our sense of smell and taste, we get headaches, and we experience extreme fatigue as our muscles are and heart or presumably getting bombarded by highly-reactive iron while simultaneously being deprived of oxygen. And it spreads its iron-based damage EVENLY throughout the lungs via our blood vessels, thus creating that non-localized ground glass look.
And, of course, by this time our innate immune system has put up an unholy war against whatever is going on. It’s cranked up our body temperature/fever in order for it to work more efficiently and also possibly cook off the virus. (Which may not be effective in this case as bats have a higher body temperature than humans with a fever and so it’s probably well adapted to that heat).
Another common symptom is the complaint of bone-level pain and aches. I would argue that’s exactly what it is, our bone marrow is working overtime to create new, uninfected red blood cells.
Serious Symptoms
If your immune system hasn’t either been strong enough or had enough time to clear out the virus before a lot of damage is done, then you start to go down the “dire” path of this disease, you may find yourself headed to the hospital, or possibly even landing in the ICU. What’s going at this point in my theory?
If your immune system hasn’t either been strong enough or had enough time to clear out the virus before a lot of damage is done, then you start to go down the “dire” path of this disease, you may find yourself headed to the hospital, or possibly even landing in the ICU. What’s going at this point in my theory?
Simply put, a lot of damage across the whole body, including any organ that gets blood (that would be pretty much all of them). In other words, I don’t view this as a disease of mostly the lungs, but rather a disease that is attacking the entire body. Yes, it started in the lungs and is probably still doing most of its viral replication in the lungs, and so they have a head start on the damage front. But it’s also attacking everything else too.


The first serious symptom is low oxygen readings. But, doctors some doctors are quite confused by something they are seeing in hospitalized patients with COVID. They are finding that many of them have shockingly low oxygen readings, but are acting pretty much normal, at least for a while. Ordinarily low (measured) oxygen levels cause patients to become incoherent, unconscious and at low enough levels death. But many of these patients seem almost normal.
What’s going on here? I believe this can be partially explained by the nature of what the virus is doing to the red blood cells. Finger based pulse oximeters work by looking at the hemoglobin to determine whether there’s oxygen atoms connected to the iron inside the red blood cell. However, it’s not there. The red blood cells have been partially or maybe completely taken over by the virus. Is this “tricking” the pulse oximeters into a false-ish reading. I’m not sure, as that’s a bit over my head. Maybe the oxygen that oxygen is still flowing loosely in the blood serum, at least for a while and perhaps it’s still doing some good, which is why we see people with “low oxygen” actually seeming more or less okay, until they aren’t. But body is also compensating for the low oxygen in the red blood cells by cranking up respiratory rates, which is an observed feature of COVID at this stage.
But seeing such low oxygen level readings, doctors do what they understand best and start hooking patients up to positive pressure ventilators. Under the, I would argue, partially false assumption that the damaged lungs need more air, in the hope of increasing oxygen levels. When in fact, forcibly adding air to the lungs could be causing more harm than good (and Business Insider). Ventilators are normally be used for lungs that are ‘tiring out’, but that doesn’t appear to be what’s happening in the vast majority of cases. Patients can inhale and exhale just fine (though with some discomfort), their blood just isn’t accepting the oxygen due to the viruses attaching to the hemoglobin. High pressure ventilation is basically just bursting the already stressed alveoli. Current statistics are showing that if you reach the point where you are hooked up to a ventilator, your chance of being disconnected from that alive is only 20%.

I would argue that rather than forcing more air into the lungs, we need to find a way to eradicate the virus from the bloods or better yet prevent them from binding with the hemoglobin in the first placeand also clean up the free radical iron an oxygen flowing around the body. Ideas for that below.
Deadly Symptoms
It seems that whether or not you die or arguably even get very sick, has to do with the race between virus multiplication (and I would argue attacking the heme) and our body’s immune response. It’s presumed that none of us have immunity to this virus (though I would argue that some do, but that’s a different article), so it’s a literal battle battle to the death between our innate immune system and it’s T-Cells, Cytokines, Macrophages and and the virus. Winner takes all. Giving our body as much time as possible win this battle is critical, which can be done through strengthening our immune system, hoping for a low dose of the virus.
It seems that whether or not you die or arguably even get very sick, has to do with the race between virus multiplication (and I would argue attacking the heme) and our body’s immune response. It’s presumed that none of us have immunity to this virus (though I would argue that some do, but that’s a different article), so it’s a literal battle battle to the death between our innate immune system and it’s T-Cells, Cytokines, Macrophages and and the virus. Winner takes all. Giving our body as much time as possible win this battle is critical, which can be done through strengthening our immune system, hoping for a low dose of the virus.
If the battle is lost, it usually results in multiple organ failure and death. Prevailing opinions are that this is due to a lack of oxygen, which makes sense, and it undoubtedly the major factor, but not because the lungs aren’t fully working, but rather because the blood can’t carry oxygen properly. In addition longer the organs have been being hammered by potent free radicals, the more likely they are to reach a tipping point and fail. Possibly exacerbated by ventilation.
It’s worth noting that this virus might actually be quite fragile if presented with an properly configured advisory. Distributed Bio is claming their “cure” can clear the virus in 20 minutes. A claim disputed by Dr. Fauci of the NIAID.
Now let’s connect the dots on risk factors
Let’s start with Blood Type: It’s now believed that some blood types lead to more dire consequences than others. Blood type A being the most harmful and O being the least. It’s interesting to note that in fact Type A blood has the highest “total iron binding capacity” and O has the lowest. So presumably with extra iron to release, extra damage occurs.
Let’s start with Blood Type: It’s now believed that some blood types lead to more dire consequences than others. Blood type A being the most harmful and O being the least. It’s interesting to note that in fact Type A blood has the highest “total iron binding capacity” and O has the lowest. So presumably with extra iron to release, extra damage occurs.
Age: This is probably due to several factors, weaker immune system which allows the virus to win the war, weaker organs that fail before the body is able to eradicate the virus. Also, general levels of iron builds up over time, this is from our food and even from what we cook on. More co-morbidities in general. Kids have the lowest level of unnecessary iron in their bodies and lowest co-morbidities.
Gender: Women have less iron in their blood due to menstruation and thus have less of the dangerous stuff flying around when it’s released from red blood cells. Not much less, but enough to possibly account for the 5–10% difference in gender mortality?
Co-morbidities like high blood pressure, diabetes and obesity obviously have caused harm to organs in advance of COVID infection and as such cause the disease to go down the dire path more easily. There’s probably more to this than I have time to research.
Treatments
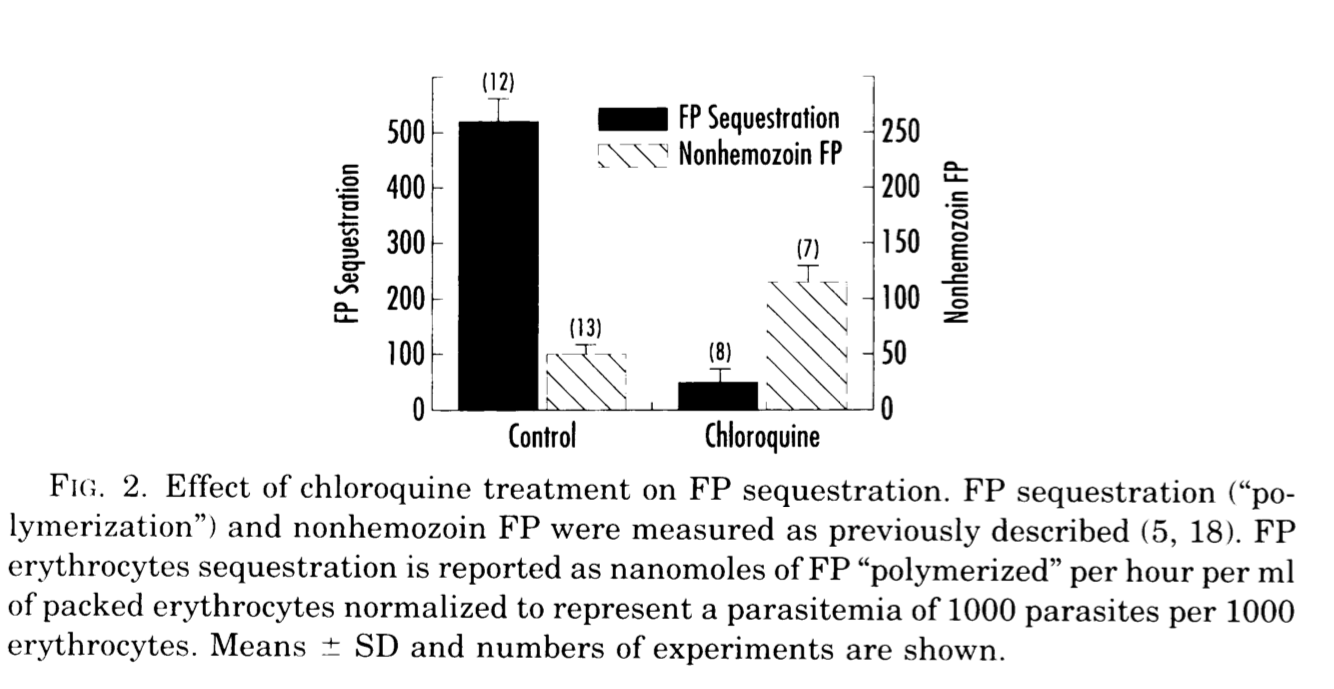
The big one is Hydroxychloroquine (HCQ) (research: Hydroxychloroquine / Chloroquine Phosphate also SARS-COV1 2004, 2005, 2008, 2009 ): As it turns out malaria is also a disease that attacks the hemoglobin of the red blood cells and HCQ blocks malaria from entering. It’s not far-fetched to assume, and there’s a lot of research to back this up, it can do the same for the coronavirus. HCQ also lowers the pH which can interfere with the virus. It may be even more effective when combined with Zinc and/or Azithromycin. Research is ongoing. Please note patients should not be taking Metformin at the same time as this regimin.
The big one is Hydroxychloroquine (HCQ) (research: Hydroxychloroquine / Chloroquine Phosphate also SARS-COV1 2004, 2005, 2008, 2009 ): As it turns out malaria is also a disease that attacks the hemoglobin of the red blood cells and HCQ blocks malaria from entering. It’s not far-fetched to assume, and there’s a lot of research to back this up, it can do the same for the coronavirus. HCQ also lowers the pH which can interfere with the virus. It may be even more effective when combined with Zinc and/or Azithromycin. Research is ongoing. Please note patients should not be taking Metformin at the same time as this regimin.
(Intravenous) Vitamin-C: Vitamin C is a powerful antioxidant that can help bind to and sweep away the iron and change the Ph of the blood to make it harder for the virus to survive. Vitamin-C has also shown promise in reducing duration of ICU stays.
If you are far enough gone, and your blood is carrying almost no oxygen at this point, a blood transfusion of fresh, uninfected red blood cells might just buy enough time for your immune system to kill of the virus before it kills you.
Other anti-virals like AIDS antivirals, Remdesivir, or Favipiravir may also help, even if it’s just to slow down the replication of the virus.
The key to treating this disease may turn out to be exactly what I’ve been saying for months now, Antivirals, Chloroquine, Zinc. And give them early, even prophylactically for those at high risk like medical workers and those of us with Type A blood.
Doctors, if this hypothesis is right, please stop treating this like you would pneumonia or ARDS. Doing so may in fact be making things worse. If you do put somebody on a ventilator, turn the PEEP (pressure) down and the oxygen up. Better yet, maybe we need to look more seriously at blood transfusions as a way to buy our immune systems more time.
In conclusion, I believe this virus has tricked us and sent us barking up the wrong tree from the beginning. If this theory can in fact be confirmed, I believe it provides a better approach to treating and/or curing this disease, and I encourage those with deeper understanding of these issues to please review the many sources presented in this document.

This is fascinating. I have been an RN for 52 years now and this sounds very promising and heading in the right direction. It makes perfect sense. I am also O- blood type and have always had a high immune system, so that makes me feel good, however, I usually run high with my iron. Very interesting please keep digging.
ReplyDeleteJoan, RN from Oregon